- 22, Apr 2026 | Khilak Budhathoki
Everest Base Camp trek vaccinations protect against 8 preventable diseases across 130 km of remote Himalayan terrain. Nepal requires no mandatory vaccines for most travelers, but Hepatitis A, Hepatitis B, Typhoid, Tetanus, Polio, Rabies, Influenza, and Cholera are medically recommended based on food contamination risk, animal exposure, and cold altitude conditions.
High altitude above 3,500 m suppresses immune function, making every infection more severe and harder to treat. Trekkers face contaminated food, unsafe water, stray dog bites, and crowded teahouse conditions in remote Khumbu terrain with no hospital access beyond Namche Bazaar. Trekking permits do not require vaccination proof. No hospital operates above Pheriche (4,371 m). Malaria tablets are not needed for the EBC route. Vaccinations for Everest Base Camp trek cost $150 to $500 USD total and prevent medical evacuation costs of $3,000 to $20,000 USD. Start your vaccination schedule 6 to 8 weeks before departure through a GP or travel medicine specialist.
Are Vaccinations Required for Everest Base Camp Trek?
Nepal does not mandate vaccinations for most travelers. No vaccine is legally required for entry unless you arrive from a Yellow Fever risk country.
The distinction is critical: legal requirement versus medical recommendation.
Nepal's government requires only one document conditionally alongside the Nepal visa for Everest Base Camp trek: a Yellow Fever vaccination certificate. This applies when you transit through or travel from countries where Yellow Fever is endemic, such as sub-Saharan Africa or tropical South America.
For all other travelers, vaccinations are medical recommendations, not entry conditions.
Medical recommendation means: unvaccinated trekkers enter Nepal legally, but face preventable illness risk across 12 to 16 days of trekking in remote mountain villages with limited healthcare access.
Sagarmatha National Park issues trekking permits without medical checks. The Khumbu Pasang Lhamu Rural Municipality collects TIMS cards without vaccination proof. No checkpoint between Lukla and Everest Base Camp verifies vaccination status.
Risk exists regardless of legal requirement. The Terai lowlands carry mosquito-borne disease. Kathmandu and Namche Bazaar carry waterborne pathogen exposure. High altitude above 3,500 m suppresses white blood cell function, reducing your body's infection response.
What Vaccines Are Recommended for Everest Base Camp Trek?
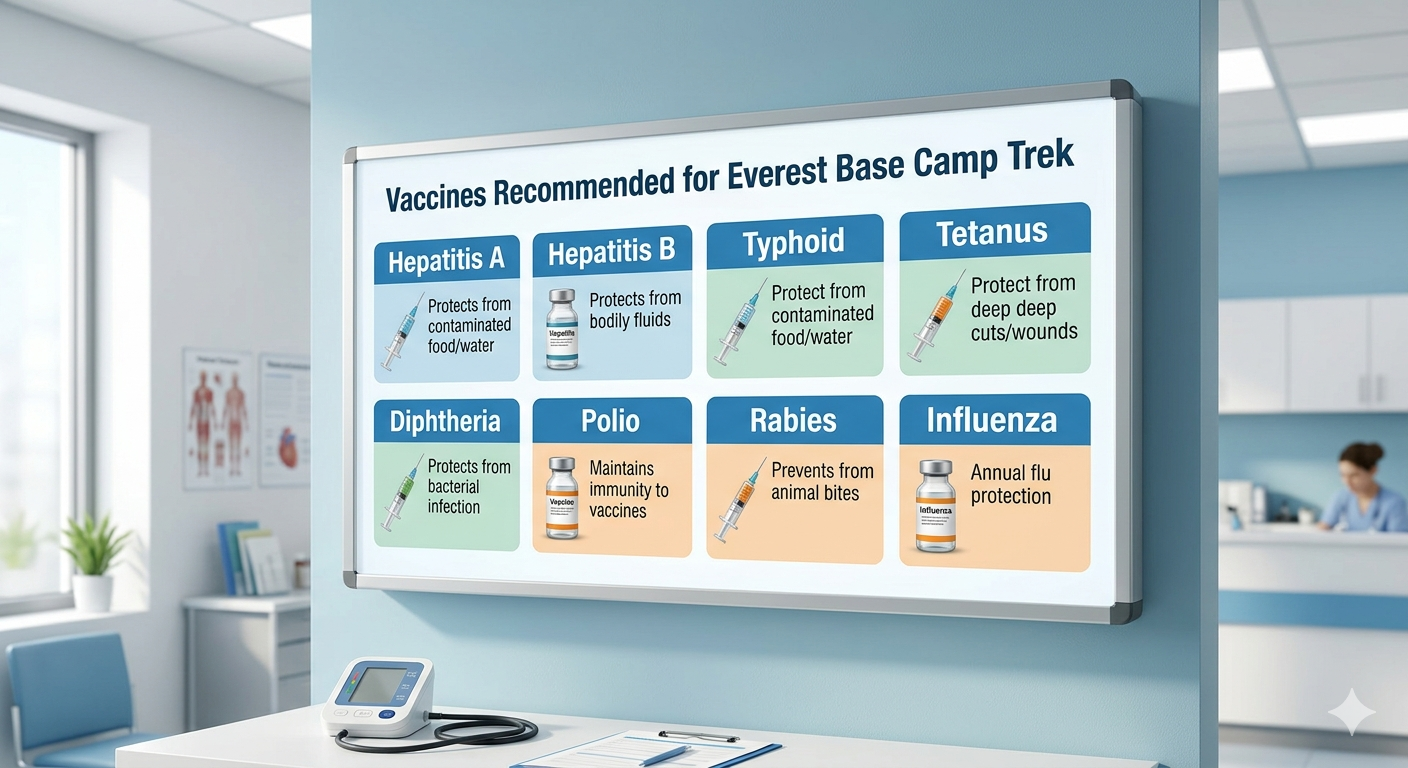
8 vaccines form the core protection protocol for Everest Base Camp trekkers. The World Health Organization and Centers for Disease Control classify these based on Nepal's disease epidemiology, trekking exposure conditions, and altitude physiology.
Vaccine selection depends on 3 factors: transmission route, geographic risk zone, and trekker exposure profile.
Do You Need Hepatitis A and B Vaccines for Everest Base Camp Trek?
Hepatitis A vaccination is strongly recommended for all Everest Base Camp trekkers. Hepatitis B vaccination is recommended for trekkers on long stays or with medical exposure risk.
Hepatitis A transmits through contaminated food and water. Nepal's rural teahouse kitchens carry high contamination risk. Hepatitis A risk is classified as high across Nepal by the CDC.
The Hepatitis A vaccine requires 2 doses. The first dose provides protection within 2 weeks. The second dose, given 6 to 12 months later, extends protection beyond 20 years.
Hepatitis B transmits through blood and body fluids. Trekkers needing medical treatment in Kathmandu clinics or Phakding health posts face exposure risk through unsterilized equipment.
The Hepatitis B vaccine requires 3 doses over 6 months. An accelerated schedule completes 3 doses in 21 days for last-minute travelers.
A combined Hepatitis A and B vaccine (Twinrix) reduces total injection appointments and is available through travel clinics.
Is Typhoid Vaccination Necessary for Everest Base Camp Trek?
Typhoid vaccination is recommended for all Everest Base Camp trekkers. Salmonella typhi transmits through contaminated food and water in Nepal's trekking corridors.
Typhoid risk is high in rural Nepal. Teahouse water sources along the Namche to Gorak Shep route carry pathogen exposure risk even when boiled.
2 vaccine types exist:
-
Injectable Vi polysaccharide vaccine: single dose, active 2 to 3 years, given at least 2 weeks before travel
-
Oral Ty21a vaccine: 4 capsules taken every other day, active 5 years, completed 1 week before travel
Typhoid vaccine effectiveness is partial, reaching 50 to 80% efficacy. Water purification with UV sterilizers or iodine tablets provides supplementary protection.
Do You Need Tetanus, Diphtheria, and Polio Boosters for EBC Trek?
Tetanus, Diphtheria, and Polio boosters are recommended if your last dose was more than 10 years ago. These are routine vaccines, not travel-specific, but remote trekking conditions increase injury risk.
Tetanus enters through wounds and cuts. Rocky terrain from Lukla to Base Camp creates blister, sprain, and laceration risk daily.
Diphtheria spreads through respiratory contact. Crowded teahouses at Namche Bazaar and Dingboche host trekkers from 40+ countries in close quarters.
Polio risk remains low but present in South Asia. A single booster dose provides full adult protection.
The Tdap combined vaccine covers Tetanus, Diphtheria, and Pertussis in one injection.
Should You Get Rabies Vaccine for Everest Base Camp Trek?
Rabies pre-exposure vaccination is recommended for Everest Base Camp trekkers spending more than 4 weeks in Nepal or trekking through rural villages. Stray dogs and monkeys in Namche Bazaar and Kathmandu carry rabies transmission risk.
Rabies fatality rate without treatment reaches nearly 100%. Post-exposure treatment requires rabies immunoglobulin (RIG), which is unavailable beyond Kathmandu.
Pre-exposure protocol: 3 doses given on Days 0, 7, and 21 or 28.
If bitten without pre-exposure vaccination: 5 post-exposure doses plus RIG required immediately.
If bitten with pre-exposure vaccination: 2 post-exposure doses required, no RIG needed.
Helicopter evacuation from Base Camp to Kathmandu for post-exposure treatment costs $3,000 to $8,000 USD without travel insurance. Pre-exposure vaccination at $150 to $300 USD total eliminates this risk.
Is Japanese Encephalitis a Risk During Everest Base Camp Trek?
Japanese Encephalitis risk is low for Everest Base Camp trekkers. Risk is present in Nepal's Terai lowland region, not in the Khumbu Himalayan trekking zone above 2,000 m.
Japanese Encephalitis transmits through Culex mosquito bites. Mosquitoes do not survive above 2,000 m altitude. Trekking routes above Lukla (2,840 m) carry no Japanese Encephalitis exposure.
Vaccination is recommended only for trekkers spending 4 or more weeks in Nepal's Terai region, Chitwan National Park, or Bardia National Park before or after the EBC trek.
The Ixiaro vaccine requires 2 doses, given 28 days apart, completed at least 1 week before Terai exposure.
Do You Need Influenza (Flu) Vaccine for High-Altitude Trekking?
Influenza vaccination is recommended for Everest Base Camp trekkers during October to April peak trekking seasons. Cold temperatures and crowded teahouse sleeping conditions accelerate influenza transmission.
High altitude above 3,500 m reduces immune response. Influenza at altitude causes more severe symptoms than at sea level. Respiratory infections are the second most common medical evacuation cause on EBC treks after Acute Mountain Sickness on the Everest Base Camp trek.
The annual flu vaccine provides seasonal protection. A single dose administered 2 weeks before departure activates full immunity.
Do You Need a Yellow Fever Vaccine for Nepal Travel?
Yellow Fever vaccination is required only for travelers arriving from Yellow Fever endemic countries. Nepal itself has no Yellow Fever risk.
The conditional requirement applies to travelers entering Nepal from sub-Saharan Africa, tropical South America, or other WHO-designated Yellow Fever risk countries. This includes transit passengers who pass through these countries within the previous 12 months.
Required documentation: an International Certificate of Vaccination or Prophylaxis (ICVP), commonly called the Yellow Card.
Without a valid ICVP and valid passport meeting the requirements for the Everest Base Camp trek when required, Nepal immigration officers can refuse entry or require immediate vaccination at port of entry.
UK travelers, US travelers, and Australian travelers flying directly to Kathmandu from their home countries do not require Yellow Fever vaccination.
Are COVID-19 Vaccinations Required for Everest Base Camp Trek?
Nepal does not currently require COVID-19 vaccination for entry or trekking permits. COVID-19 vaccination is optional personal health protection.
Nepal removed mandatory COVID-19 documentation requirements. Trekking permits for Sagarmatha National Park, TIMS cards, and Khumbu conservation fees do not require proof of COVID-19 vaccination.
COVID-19 risk at high altitude warrants individual assessment. Cold temperatures, reduced oxygen availability, and crowded teahouse conditions create respiratory transmission conditions. Trekkers with pre-existing respiratory or cardiovascular conditions benefit from full COVID-19 vaccination before travel.
Consult your General Practitioner (GP) or travel medicine specialist for a personal risk assessment based on your vaccination history and health profile.
When Should You Get Vaccinated Before Everest Base Camp Trek?
Start vaccinations 6 to 8 weeks before your 14-day guided Khumbu Himalayan expedition departure date. This window allows time for multi-dose vaccines to complete and immunity to develop.
Immunity develops after a time delay, not immediately after injection. Hepatitis A provides partial protection after 2 weeks. Typhoid injectable vaccine activates in 2 weeks. Rabies pre-exposure course requires 3 to 4 weeks.
Vaccination timeline by vaccine:
-
Hepatitis A: First dose at 6 weeks, second dose 6 to 12 months later
-
Typhoid injectable: Single dose at 2 weeks minimum
-
Typhoid oral: Complete 4-dose course 1 week before travel
-
Rabies: Day 0, Day 7, Day 21 or 28 (requires 4 weeks minimum)
-
Tetanus/Tdap: Single booster, effective immediately
-
Influenza: Single dose, 2 weeks before travel
-
Hepatitis B: 3 doses over 6 months (accelerated: 21 days)
Last-minute travelers departing in under 4 weeks can still receive Hepatitis A, Typhoid injectable, Tetanus, and Influenza vaccines with partial protection. Rabies and Hepatitis B require an accelerated schedule arranged through a travel medicine specialist.
What Health Risks Do Vaccinations Help Prevent on the EBC Trek?
Vaccinations protect against 4 primary risk categories on the Everest Base Camp trek: waterborne disease, foodborne disease, vector-borne disease, and animal-contact disease.
Food and water contamination on the Everest Base Camp trek is the highest daily exposure risk. Teahouse kitchens in Namche Bazaar, Tengboche, Dingboche, Lobuche, and Gorak Shep use water from glacial streams and local wells. Untreated water carries Salmonella, E. coli, Giardia lamblia, Campylobacter, and Cryptosporidium. Traveler's diarrhea probability on Nepal treks reaches 30 to 50%.
Remote medical access limitation amplifies every illness. The nearest hospital with surgical capacity is CIWEC Hospital in Kathmandu. Phakding and Pheriche have health posts with basic first aid. Above Namche Bazaar, the Himalayan Rescue Association aid post at Pheriche (4,371 m) handles altitude emergencies only. No clinic operates above Lobuche (4,940 m).
Cold and altitude immune interaction creates a compounding risk. Altitude above 3,500 m reduces white blood cell count and function. Hypoxia at 5,364 m (Base Camp elevation) suppresses inflammatory response. Infections that resolve in 3 days at sea level become 7 to 10 day illnesses at altitude. Respiratory infections above 4,000 m carry pneumonia risk requiring evacuation.
Do You Need Malaria Prevention for Everest Base Camp Trek?
Malaria prophylaxis is not required for Everest Base Camp trekkers. Malaria-carrying Anopheles mosquitoes do not survive above 1,200 m altitude.
The entire EBC trekking route operates above 2,840 m. Lukla, the trek starting point, sits at 2,840 m. No malaria transmission risk exists along the Namche, Tengboche, Dingboche, Lobuche, or Gorak Shep route.
Malaria risk is present in Nepal's Terai lowlands, including Chitwan District and Bardiya District, below 1,200 m. Trekkers spending time in Terai before or after the EBC trek should discuss Plasmodium vivax and Plasmodium falciparum prophylaxis with a travel medicine specialist.
Prophylaxis options for Terai exposure: Atovaquone-proguanil (Malarone), Doxycycline, or Mefloquine. Each requires prescription and individual assessment.
Kathmandu (1,400 m) sits above the malaria transmission zone. No prophylaxis is needed for Kathmandu pre-trek or post-trek stays.
What Medications Should You Take Alongside Vaccinations for EBC Trek?
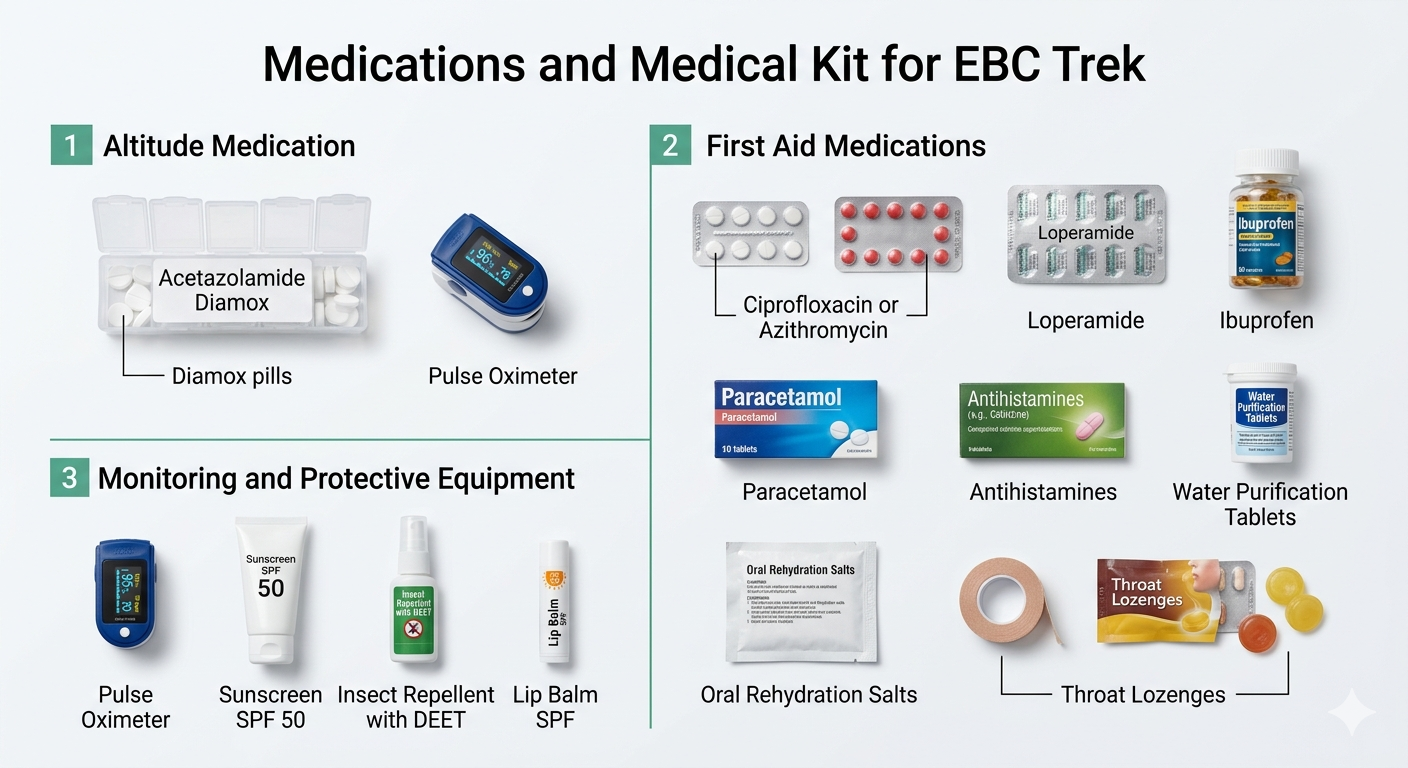
5 medication categories support health protection alongside vaccinations on the EBC trek: altitude medication, antibiotic therapy, gastrointestinal treatment, pain management, and antihistamines.
Should You Take Acetazolamide (Diamox) for Altitude Sickness?
Acetazolamide (Diamox) for the Everest Base Camp trek treats and prevents Acute Mountain Sickness (AMS). AMS affects 50 to 75% of trekkers above 3,500 m without adequate acclimatization.
Diamox works by stimulating faster breathing, which increases blood oxygen saturation. It reduces AMS symptoms including headache, nausea, and dizziness.
Preventive dose: 125 mg twice daily, starting 1 to 2 days before significant altitude gain.
Treatment dose: 250 mg twice daily until symptoms resolve or descent begins.
Diamox requires a prescription. Consult your GP or travel medicine specialist before departure. Sulfonamide allergy is a contraindication. Common side effects include increased urination and tingling in fingers and toes.
A pulse oximeter measures blood oxygen saturation at altitude. Normal readings above 90% are acceptable at altitude. Readings below 85% indicate serious altitude illness requiring descent.
What First Aid and Preventive Medicines Should You Carry for EBC Trek?
A complete EBC trek medical kit includes 8 essential medications and 4 monitoring tools.
Medications:
-
Ciprofloxacin or Azithromycin: prescription antibiotic for severe traveler's diarrhea or respiratory infection
-
Loperamide: controls diarrhea symptoms during trekking days
-
Ibuprofen: reduces inflammation, headache, and muscle pain
-
Paracetamol: fever and pain management, safer at altitude than ibuprofen for kidney function
-
Antihistamines: allergic reaction management
-
Water purification tablets: iodine or chlorine based for emergency water treatment
-
Oral rehydration salts: replaces electrolytes lost through diarrhea or dehydration
-
Throat lozenges: manages respiratory irritation from cold, dry air
Monitoring and protective equipment:
-
Pulse oximeter: tracks blood oxygen saturation daily above 3,500 m
-
Sunscreen SPF 50: UV exposure increases 10% per 1,000 m altitude gain
-
Insect repellent with DEET: Terai and Kathmandu mosquito protection
-
Lip balm SPF: sun and cold wind protection above treeline
Do You Need Proof of Vaccination for Everest Base Camp Trek Permits?
No vaccination proof is required for any Everest Base Camp trekking permit. Sagarmatha National Park entry, TIMS card, and Khumbu Pasang Lhamu Rural Municipality conservation fees do not include medical documentation checks.
The permit process at Monjo checkpoint verifies: passport, Sagarmatha National Park permit (NPR 3,000 for SAARC nationals, NPR 3,000 USD equivalent for others), and TIMS card. No health documents are requested.
The single exception: Yellow Fever vaccination certificate (ICVP) is checked at Tribhuvan International Airport immigration for travelers from Yellow Fever endemic countries. This is an immigration requirement, not a trekking permit requirement.
Travel insurance documentation is separate from vaccination proof and belongs in your travel documents checklist for the Everest Base Camp trek. Trekking companies and helicopter rescue operators require proof of travel insurance with high-altitude evacuation coverage above 6,000 m. This is a financial document, not a medical one.
Can You Trek to Everest Base Camp Without Vaccinations?
Trekking Everest Base Camp without vaccinations is legally permitted but medically inadvisable. No checkpoint refuses entry to unvaccinated trekkers.
The practical reality: unvaccinated trekkers face avoidable illness risk across 130 km of remote terrain. Hepatitis A contracted in a Namche teahouse causes 2 to 6 weeks of liver inflammation. Typhoid fever causes 1 to 4 weeks of fever, weakness, and intestinal complications. Rabies without post-exposure treatment is fatal.
Medical infrastructure limitations define the risk. Above Namche Bazaar (3,440 m), no pharmacy carries rabies immunoglobulin. No clinic above Pheriche (4,371 m) treats serious infections. Helicopter evacuation to Kathmandu costs $3,000 to $8,000 USD per flight.
Trekking without vaccines shifts manageable prevention costs (vaccine course: $150 to $500 USD) into potential emergency costs ($3,000 to $20,000 USD) or permanent health consequences.
What Vaccinations Are Recommended Based on Trek Duration and Season?
Trek duration and season determine 3 vaccination priority levels for Everest Base Camp.
Short trek (12 to 16 days, standard route through the Sagarmatha and Khumbu trekking region): Hepatitis A, Typhoid, Tetanus booster, and Influenza form the minimum protection set. Rabies is recommended but not critical for trekkers with zero animal contact risk.
Long trek or extended Nepal stay (4 or more weeks): Full vaccine protocol including Hepatitis B and Rabies pre-exposure is medically recommended. Extended rural and village exposure increases animal bite and blood contact probability.
Season-specific adjustments:
October to November (peak autumn season): Highest trekker density in teahouses increases Influenza and respiratory infection transmission. Full vaccine protocol recommended.
March to May (peak spring season): Warmer lower-altitude temperatures increase waterborne pathogen activity. Typhoid and Hepatitis A vaccines are especially important.
June to September (monsoon season): Kathmandu and lower trail sections see increased mosquito activity. Japanese Encephalitis risk rises in Terai. Trekkers beginning in Terai before monsoon EBC attempts need Japanese Encephalitis assessment.
December to February (winter season): Extreme cold reduces waterborne transmission but increases respiratory illness severity at altitude. Influenza vaccine is critical.
What Should You Discuss with a Travel Clinic Before Everest Base Camp Trek?
Consult a travel medicine specialist or GP at least 6 to 8 weeks before departure. A travel clinic risk assessment covers 5 areas specific to Everest Base Camp preparation.
Personal health profile review: Pre-existing cardiovascular or respiratory conditions affect both vaccine selection and altitude risk. Sulfonamide allergy contraindicates Diamox. Pregnancy changes vaccine recommendations for live vaccines including oral Typhoid.
Vaccination history audit: Many adults hold partial Hepatitis B or Polio immunity from childhood schedules. A serology test (antibody test) confirms existing immunity and prevents unnecessary re-vaccination.
Region-specific risk assessment: Travel itinerary before and after EBC determines Japanese Encephalitis and Malaria exposure windows. Chitwan safari before EBC trek changes the prophylaxis protocol.
Prescription medication assessment: Diamox, Ciprofloxacin, and Azithromycin require prescription. A travel clinic issues these in a single appointment with instructions for self-treatment protocols on the trail.
Insurance and evacuation planning: Travel insurance with emergency helicopter evacuation coverage above 6,000 m is non-negotiable for EBC trekkers. Your travel clinic can provide written medical documentation for insurance claims.
Travel clinics in the UK (MASTA, Nomad, GP travel services), US (CDC-affiliated travel clinics), and Australia (Travel Medicine Alliance) provide full EBC pre-travel consultations.
FAQs About Everest Base Camp Trek Vaccinations
What vaccines do you need for Everest Base Camp trek?
8 vaccines are recommended for Everest Base Camp trek: Hepatitis A, Hepatitis B, Typhoid, Tetanus, Diphtheria, Polio, Rabies, and Influenza. Cholera is a secondary recommendation. Yellow Fever is required only for travelers from endemic countries. Start vaccinations 6 to 8 weeks before departure.
Are vaccinations mandatory for Nepal travel?
No vaccinations are legally mandatory for Nepal travel except Yellow Fever for travelers arriving from endemic countries. All other vaccines are medical recommendations based on disease exposure risk in Nepal's trekking regions.
Can you trek Everest Base Camp without vaccines?
Trekking Everest Base Camp without vaccinations is legal but risky. No checkpoint requires vaccination proof. Unvaccinated trekkers face Hepatitis A, Typhoid, Tetanus, and Rabies exposure with no hospital access beyond Namche Bazaar and evacuation costs reaching $8,000 USD.
Do I need malaria tablets for Everest Base Camp trek?
No malaria tablets are needed for Everest Base Camp trek. The entire EBC route operates above 2,840 m. Malaria-carrying mosquitoes do not survive above 1,200 m. Malaria prophylaxis is needed only for Terai lowland travel before or after the trek.
Is yellow fever vaccine required for Nepal visa?
Yellow Fever vaccine is not required for Nepal visa. It is required only at airport immigration for travelers arriving from sub-Saharan Africa, tropical South America, or other WHO-designated Yellow Fever endemic countries. The required document is an ICVP (Yellow Card), not a visa condition.
How early should I get vaccinated before EBC trek?
Start vaccinations 6 to 8 weeks before EBC trek departure. Rabies pre-exposure requires 4 weeks minimum for 3 doses. Hepatitis A requires 2 weeks for initial protection. Hepatitis B full course requires 6 months (accelerated schedule: 21 days). Typhoid injectable requires 2 weeks before travel.
More About Author

Khilak Budhathoki
Travel Director
Khilak Budhathoki is the co-founder and lead trekking guide at Himalaya Trekking Nepal, a locally owned and operated adventure company based in Kathmandu. Born and raised in the foothills of Nepal, Khilak developed a deep love for the mountains from an early age. With over a deca...

USD$1,600 pp
Our Recommendation
Related Blogs


Jan 25, 2026
Annapurna I – 10th Highest Mountain in the World

Dec 15, 2025
Annapurna Base Camp Packing List – ABC Trek Guide
